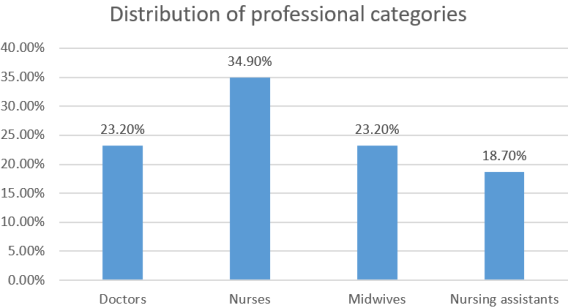
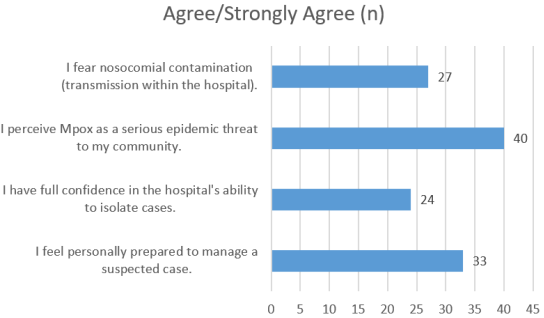
Introduction. Monkeypox (MPOX) was declared a Public Health Emergency of International Concern (PHEIC) in 2022. In Benin, early identification of suspected cases by Frontline Health Workers (FHWs) in Emergency Departments (ED) is vital to stopping the chain of transmission and preventing community and nosocomial spread. This study aimed to assess the capacity of FHWs to identify Mpox in three strategic hospital facilities in Benin. Methods. We conducted a cross-sectional descriptive study with a qualitative component from February to May 2025 in three hospitals (Oueme Plateau Departmental Hospital Center, Zou Departmental Hospital Center, and Save Zone Hospital). A total of 43 FHWs (physicians, nurses, midwives, nursing assistants) were selected using a non-probability purposive sampling technique. Data on knowledge, attitudes, and practices (KAP) were collected via semi-structured interviews and analyzed using descriptive statistics. Institutional Standard Operating Procedures (SOPs) were assessed via document review. Results. The majority of participants were nurses (34.9%), with an average emergency department seniority of 4.1 years. Overall, 83.7% of staff demonstrated "good" theoretical knowledge for identifying suspected cases. However, only 65.1% explicitly identified sexual transmission as a route of infection, with a notable disparity between physicians (90%) and nursing assistants (37.5%). While risk perception was high (93.0%), only 55.8% trusted the hospital's isolation capacity, and 58.1% reported constant Personal Protective Equipment (PPE) availability. Discrepancies were found in institutional preparedness, with one hospital lacking updated SOPs. Conclusion. Frontline healthcare workers have a high theoretical ability to identify MPOX, but operational capacity is hindered by logistical challenges and gaps in knowledge regarding sexual transmission among non-medical staff. Limitations include the small sample size.
| Published in | World Journal of Public Health (Volume 10, Issue 4) |
| DOI | 10.11648/j.wjph.20251004.25 |
| Page(s) | 580-585 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
MPOX, frontline Healthcare Workers, Emergency Department, Benin
Key Mpox Symptom | Workers Who Identified It (n) | Percentage (%) |
|---|---|---|
Vesicular/pustular skin rash | 39 | 90.7 |
Lymphadenopathy | 37 | 86.0 |
Fever and headache | 34 | 79.1 |
Mode of Transmission | Workers Who Identified It (n) | Percentage (%) |
|---|---|---|
Direct contact with lesions | 42 | 97.7 |
Respiratory droplets | 35 | 81.4 |
Contaminated fomites | 30 | 69.8 |
Sexual transmission | 28 | 65.1 |
Professional Category | Total (n) | Identified Sexual Transmission n (%) | Did Not Identify n (%) |
|---|---|---|---|
Doctors | 10 | 9 (90.0) | 1 (10.0) |
Nurses | 15 | 9 (60.0) | 6 (40.0) |
Midwives | 10 | 6 (60.0) | 4 (40.0) |
Nursing Assistants | 8 | 3 (37.5) | 5 (62.5) |
Total | 43 | 28 (65.1) | 15 (34.9) |
CDC | Centers for Disease Control and Prevention |
ED | Emergency Department |
ETAT | Emergency Triage Assessment and Treatment |
FHW | Frontline Health Worker |
IPC | Infection Prevention and Control |
KAP | Knowledge, Attitudes, and Practices |
PHEIC | Public Health Emergency of International Concern |
PPE | Personal Protective Equipment |
SOP | Standard Operating Procedure |
WHO | World Health Organization |
| [1] | WHO. Mpox outbreaks: situation update. Geneva: WHO; 2023. |
| [2] | WHO. Multi-country outbreak of monkeypox, 2022. Geneva: WHO; 2022. |
| [3] | Thornhill JP, et al. Mpox Infection in Humans across 16 Countries. N Engl J Med. 2022; 387(18): 1668-1678. |
| [4] | Petersen E, et al. Mpox – The emergence of a poxvirus in non-endemic countries. Int J Infect Dis. 2022; 122: 105–111. |
| [5] | Bunge EM, et al. The changing epidemiology of Mpox: a systematic review. Lancet Infect Dis. 2022; 22(6): 868-877. |
| [6] | Yinka-Ogunleye A, et al. Outbreak of human monkeypox in Nigeria. Lancet Infect Dis. 2018; 18(8): 834–836. |
| [7] | ANSE. Annual surveillance report of epidemic-prone diseases in Benin. Cotonou: Ministry of Health; 2024. |
| [8] | Okeke OE, Ajayi OB. Challenges of cross-border health surveillance in West Africa. J Glob Health Perspect. 2023; 7(2): 55-68. |
| [9] | Gostin LO, Phelan AL. After COVID-19—A convention on global health security. N Engl J Med. 2022; 387(18): 1639-1642. |
| [10] | Lado MD. Role of ED personnel in identification of zoonoses. J Acute Med. 2023; 15(3): 101-108. |
| [11] | Ministry of Health. National directives for managing eruptive diseases. Cotonou: MS; 2023. |
| [12] | Fine PEM, et al. Herd immunity in the eradication of monkeypox. Int J Epidemiol. 1988; 17(4): 939–949. |
| [13] | Ilori T, Obadare RA. Assessment of FHWs' knowledge regarding Mpox in Nigeria. BMC Public Health. 2024; 24(1): 320. |
| [14] | Kulkarni A, Gupta A. Risk of nosocomial transmission of Mpox. Infect Control Hosp Epidemiol. 2022; 43(11): 1438-1444. |
| [15] | U.S. CDC. Strengthening health systems in West Africa. Atlanta: CDC; 2023. |
| [16] | Lawani AA, Zossou EF. Analysis of the referral-evacuation system in Benin. Rev Ben Sante Pub. 2024; 10(1): 12-25. |
| [17] | Patton MQ. Qualitative research & evaluation methods (4th ed.). Los Angeles: Sage; 2015. |
| [18] | WHO. ETAT guidelines for frontline workers. Geneva: WHO; 2024. |
| [19] | Tettey J. Standardization of infectious disease protocols. Health Policy Plan. 2023; 38(7): 779-787. |
| [20] | Guest G, et al. Applied thematic analysis. Los Angeles: Sage; 2012. |
| [21] | Adedokun SA, Bamidele TL. Preparedness of FHWs for emerging diseases. Afr J Infect Dis. 2022; 16(4): 112-120. |
| [22] | Kéké NF, et al. Knowledge of Mpox among health workers in Benin. Int Health Policy Rev. 2025; 12(1): 45-53. |
| [23] | Mitjà O, et al. Mpox: confronting a multi-region outbreak. Lancet. 2022; 400(10352): 523-525. |
| [24] | Oladejo AE, et al. Knowledge of Mpox among medical students in Nigeria. Infect Dis Rep. 2023; 15(2): 269–277. |
| [25] | Nkengasong JN. COVID-19 in Africa: the good, the bad, and the ugly. Lancet. 2020; 395(10241): 1845-1847. |
| [26] | Africa CDC. Framework for harmonizing PHEOCs in Africa. Addis Ababa: Africa CDC; 2023. |
| [27] | Jonas OB, Ayayi TM. Role of SOPs during infectious disease outbreaks. J Qual Health Manag. 2023; 14(4): 211-220. |
| [28] | Rudolph JW, et al. Learning in simulated crises. Simul Healthc. 2007; 2(1): 46-51. |
| [29] | Mauldin MR, et al. MPXV-Specific serologic assays. Emerg Infect Dis. 2018; 24(12): 2315-2319. |
| [30] | Siegel JD, et al. 2007 Guideline for Isolation Precautions. Am J Infect Control. 2007; 35(10): S65-S164. |
APA Style
Romeo, P. S. G., Rose, M., Colette, A., Jennifer, O., Badirou, A. (2025). Assessment of Frontline Health Workers’ Capacity for Mpox Case Identification in Emergency Departments of Benin. World Journal of Public Health, 10(4), 580-585. https://doi.org/10.11648/j.wjph.20251004.25
ACS Style
Romeo, P. S. G.; Rose, M.; Colette, A.; Jennifer, O.; Badirou, A. Assessment of Frontline Health Workers’ Capacity for Mpox Case Identification in Emergency Departments of Benin. World J. Public Health 2025, 10(4), 580-585. doi: 10.11648/j.wjph.20251004.25
AMA Style
Romeo PSG, Rose M, Colette A, Jennifer O, Badirou A. Assessment of Frontline Health Workers’ Capacity for Mpox Case Identification in Emergency Departments of Benin. World J Public Health. 2025;10(4):580-585. doi: 10.11648/j.wjph.20251004.25
@article{10.11648/j.wjph.20251004.25,
author = {Padonou Sètondji Geraud Romeo and Mikponhoue Rose and Azandjeme Colette and Olofindji Jennifer and Aguemon Badirou},
title = {Assessment of Frontline Health Workers’ Capacity for Mpox Case Identification in Emergency Departments of Benin},
journal = {World Journal of Public Health},
volume = {10},
number = {4},
pages = {580-585},
doi = {10.11648/j.wjph.20251004.25},
url = {https://doi.org/10.11648/j.wjph.20251004.25},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251004.25},
abstract = {Introduction. Monkeypox (MPOX) was declared a Public Health Emergency of International Concern (PHEIC) in 2022. In Benin, early identification of suspected cases by Frontline Health Workers (FHWs) in Emergency Departments (ED) is vital to stopping the chain of transmission and preventing community and nosocomial spread. This study aimed to assess the capacity of FHWs to identify Mpox in three strategic hospital facilities in Benin. Methods. We conducted a cross-sectional descriptive study with a qualitative component from February to May 2025 in three hospitals (Oueme Plateau Departmental Hospital Center, Zou Departmental Hospital Center, and Save Zone Hospital). A total of 43 FHWs (physicians, nurses, midwives, nursing assistants) were selected using a non-probability purposive sampling technique. Data on knowledge, attitudes, and practices (KAP) were collected via semi-structured interviews and analyzed using descriptive statistics. Institutional Standard Operating Procedures (SOPs) were assessed via document review. Results. The majority of participants were nurses (34.9%), with an average emergency department seniority of 4.1 years. Overall, 83.7% of staff demonstrated "good" theoretical knowledge for identifying suspected cases. However, only 65.1% explicitly identified sexual transmission as a route of infection, with a notable disparity between physicians (90%) and nursing assistants (37.5%). While risk perception was high (93.0%), only 55.8% trusted the hospital's isolation capacity, and 58.1% reported constant Personal Protective Equipment (PPE) availability. Discrepancies were found in institutional preparedness, with one hospital lacking updated SOPs. Conclusion. Frontline healthcare workers have a high theoretical ability to identify MPOX, but operational capacity is hindered by logistical challenges and gaps in knowledge regarding sexual transmission among non-medical staff. Limitations include the small sample size.},
year = {2025}
}
TY - JOUR T1 - Assessment of Frontline Health Workers’ Capacity for Mpox Case Identification in Emergency Departments of Benin AU - Padonou Sètondji Geraud Romeo AU - Mikponhoue Rose AU - Azandjeme Colette AU - Olofindji Jennifer AU - Aguemon Badirou Y1 - 2025/12/29 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251004.25 DO - 10.11648/j.wjph.20251004.25 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 580 EP - 585 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251004.25 AB - Introduction. Monkeypox (MPOX) was declared a Public Health Emergency of International Concern (PHEIC) in 2022. In Benin, early identification of suspected cases by Frontline Health Workers (FHWs) in Emergency Departments (ED) is vital to stopping the chain of transmission and preventing community and nosocomial spread. This study aimed to assess the capacity of FHWs to identify Mpox in three strategic hospital facilities in Benin. Methods. We conducted a cross-sectional descriptive study with a qualitative component from February to May 2025 in three hospitals (Oueme Plateau Departmental Hospital Center, Zou Departmental Hospital Center, and Save Zone Hospital). A total of 43 FHWs (physicians, nurses, midwives, nursing assistants) were selected using a non-probability purposive sampling technique. Data on knowledge, attitudes, and practices (KAP) were collected via semi-structured interviews and analyzed using descriptive statistics. Institutional Standard Operating Procedures (SOPs) were assessed via document review. Results. The majority of participants were nurses (34.9%), with an average emergency department seniority of 4.1 years. Overall, 83.7% of staff demonstrated "good" theoretical knowledge for identifying suspected cases. However, only 65.1% explicitly identified sexual transmission as a route of infection, with a notable disparity between physicians (90%) and nursing assistants (37.5%). While risk perception was high (93.0%), only 55.8% trusted the hospital's isolation capacity, and 58.1% reported constant Personal Protective Equipment (PPE) availability. Discrepancies were found in institutional preparedness, with one hospital lacking updated SOPs. Conclusion. Frontline healthcare workers have a high theoretical ability to identify MPOX, but operational capacity is hindered by logistical challenges and gaps in knowledge regarding sexual transmission among non-medical staff. Limitations include the small sample size. VL - 10 IS - 4 ER -
Department of Public Health, University of Abomey-Calavi, Cotonou, Benin
Occupational Health Teaching and Research Unit, University of Abomey-Calavi, Cotonou, Benin
Regional Institute of Public Health, University of Abomey-Calavi, Ouidah, Benin
Faculty of Health Sciences, University of Abomey-Calavi, Cotonou, Benin
Department of Public Health, University of Abomey-Calavi, Cotonou, Benin