Background: The growing burden of multimorbidity, which is the occurrence of two or more chronic conditions simultaneously in an individual is a great burden on the healthcare system of Kenya that is already defined by unequal distribution of resources and access to specialists. The solution to this gap may be found in telemedicine, but due to the dependency on centralized cloud computing, the effectiveness in the context of the resources-constrained environment is critically impaired. This dependence leads to chronic problems such as unreliable internet connection, power connectivity issues, large data latency making real-time intervention difficulty, excessive bandwidth prices, and, ultimately, piecemeal care of the multimorbid patients. Methods: The study employed the use of a combination of various approaches as it started with an extensive analysis of the current state of telemedicine and its limitation in managing multimorbidity both globally and locally. Then, an architectural framework of a conceptual edge-based framework was designed that defined the primary elements of local data processing, offline functionality, and real-time clinical decision support. Results: This study developed a new, edge-computing telemedical architecture that moves vital data processing and storage operations out of the cloud and on to local edge nodes (edge devices) at the point of care. The main aim was to develop a more robust, effective and responsive telehealth system that will be able to work efficiently even in low-connectivity settings. The possible effect of this framework was compared to the key performance indicators showing that there was a substantial theoretical reduction in the latency of data transmission and the bandwidth used. Moreover, the telemedical model is projected to improve continuity and coordination of care through the processing and acting of critical patient data about IoT devices such as blood pressure, glucose monitoring locally even when the internet is unavailable. Conclusion: Integration of edge computing is a feasible and strategic solution to the basic infrastructural constraints of cloud-based telemedicine in Kenya. The suggested model does not only overcome technical obstacles of connectivity and cost, but also presents a foundational framework of scalable, patient-centered and integrated care to the increasing population of multimorbid patients.
| Published in | World Journal of Public Health (Volume 10, Issue 4) |
| DOI | 10.11648/j.wjph.20251004.26 |
| Page(s) | 586-600 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Edge Computing, Multimorbidity, Healthcare Access, Kenya, Digital Health, IoT, Home-Care, Telemedicine
Challenge Dimension | Simulated Parameter | Frequency | Implication for Healthcare Access |
|---|---|---|---|
Network Reliability | System Downtime | 28% | Care interruptions, missed alerts, unreliable service delivery. |
Network Performance | Average Latency | 1750 ms | Delayed clinical decisions, slow response to crises. |
Financial Sustainability | Monthly Data Cost/50 patients’ lot | Ksh.312,500 P.m | Financially unsustainable for most facilities, limiting scale. |
Key performance indicator (KPI) | Cloud-based model | Edge-based model | Improvement | Practical implication |
|---|---|---|---|---|
Total Bandwidth Used | 62.5 GB | 4.38 GB | 93% Reduction | Drastic reduction in operational data costs. |
Average Data Latency | 1750 ms | 50 ms | 97% Reduction | Enables real-time, life-saving clinical alerts. |
Data Offload to Cloud | 100% | 7% | 93% Reduction | Minimizes dependency on continuous connectivity. |
Service Availability | 72% | 100% (Local) | 28% Increase | Guarantees continuous monitoring, even offline. |
OOA | Object-Oriented Analysis and Design |
NCDs | Non-communicable Diseases |
ITU | International Telecommunication Union |
KDHS | Kenya Demographic and Health Survey |
RPM | Remote patient Monitoring |
EHR | Electronic Health Records |
AI | Artificial Intelligence |
KNBS | Kenya National Bureau of Statistics |
ML | Machine Learning |
SDGs | Sustainable Development Goals |
| [1] | Boikanyo, K., Zungeru, A. M., Sigweni, B., Yahya, A., & Lebekwe, C. (2023). Remote patient monitoring systems: Applications, architecture, and challenges. Scientific African, 20. |
| [2] | Fulmer, T., Reuben, D. B., Auerbach, J., Fick, D. M., Galambos, C., & Johnson, K. S. (2021). Actualizing better health and health care for older adults. Health Affairs, 40(2), 219-225. |
| [3] | Johnson, A. E. W., Bulgarelli, L., Shen, L., Gayles, A., Shammout, A., Horng, S., Pollard, T. J., Hao, S., Moody, B., Gow, B., Lehman, L. H., Celi, L. A., & Mark, R. G. (2023). MIMIC-IV, a freely accessible electronic health record dataset. Scientific Data, 10(1), 1. |
| [4] | KAHVECİ, K., KOÇ, O., & AKSAKAL, H. (2020). Home-based Palliative Care. Bezmialem Science, 8(1), 73-80. |
| [5] | Li, C., Wang, J., Wang, S., & Zhang, Y. (2024). A review of IoT applications in healthcare. Neurocomputing, 565, 127017. |
| [6] | Mayo clinic. (2021). Mayo Clinic study highlights development of remote patient monitoring program during COVID-19 pandemic. |
| [7] | Mohamed, S. F., Haregu, T. N., Uthman, O. A., Khayeka-Wandabwa, C., Muthuri, S. K., Asiki, G., Kyobutungi, C., & Gill, P. (2021a). Multimorbidity from chronic conditions among adults in urban slums: The awi-gen nairobi site study findings. Global Heart, 16(1). |
| [8] | Neußner, O. (2021). Early warning alerts for extreme natural hazard events: A review of worldwide practices. International Journal of Disaster Risk Reduction, 60, 102295. |
| [9] | Rana, Md. S., & Shuford, J. (2024). AI in Healthcare: Transforming Patient Care through Predictive Analytics and Decision Support Systems. Journal of Artificial Intelligence General Science (JAIGS), 1(1). |
| [10] | Satyanarayanan, M. (2017). The emergence of edge computing. Computer, 50(1), 30-39. |
| [11] | Schmidt, M., Schmidt, S. A. J., Adelborg, K., Sundbøll, J., Laugesen, K., Ehrenstein, V., & Sørensen, H. T. (2019). The Danish health care system and epidemiological research: From health care contacts to database records. Clinical Epidemiology, 11, 563-591. |
| [12] | Schweitzer, A.-M., Dišković, A., Krongauz, V., Newman, J., Tomažič, J., & Yancheva, N. (2023). Addressing HIV stigma in healthcare, community, and legislative settings in Central and Eastern Europe. AIDS Research and Therapy, 20(1), 87. |
| [13] | Zalte-Gaikwad, S. S., Zalte, S., Patil, M., Tone, S., & Randive, N. (n.d.). Edge Computing Technology: An Overview. Asian Journal of Organic & Medicinal Chemistry, 7(1). |
APA Style
Kapkiyai, A. K., Njuki, S. K., Ng’ang’a, N. N., Okeyo, I. (2025). Edge-Based Telemedical Architecture Integrating Edge Devices and Lightweight AI for Healthcare in Kenya. World Journal of Public Health, 10(4), 586-600. https://doi.org/10.11648/j.wjph.20251004.26
ACS Style
Kapkiyai, A. K.; Njuki, S. K.; Ng’ang’a, N. N.; Okeyo, I. Edge-Based Telemedical Architecture Integrating Edge Devices and Lightweight AI for Healthcare in Kenya. World J. Public Health 2025, 10(4), 586-600. doi: 10.11648/j.wjph.20251004.26
AMA Style
Kapkiyai AK, Njuki SK, Ng’ang’a NN, Okeyo I. Edge-Based Telemedical Architecture Integrating Edge Devices and Lightweight AI for Healthcare in Kenya. World J Public Health. 2025;10(4):586-600. doi: 10.11648/j.wjph.20251004.26
@article{10.11648/j.wjph.20251004.26,
author = {Askher Kipkoech Kapkiyai and Samson Kabangu Njuki and Njeri Ngaruiya Ng’ang’a and Isaac Okeyo},
title = {Edge-Based Telemedical Architecture Integrating Edge Devices and Lightweight AI for Healthcare in Kenya},
journal = {World Journal of Public Health},
volume = {10},
number = {4},
pages = {586-600},
doi = {10.11648/j.wjph.20251004.26},
url = {https://doi.org/10.11648/j.wjph.20251004.26},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251004.26},
abstract = {Background: The growing burden of multimorbidity, which is the occurrence of two or more chronic conditions simultaneously in an individual is a great burden on the healthcare system of Kenya that is already defined by unequal distribution of resources and access to specialists. The solution to this gap may be found in telemedicine, but due to the dependency on centralized cloud computing, the effectiveness in the context of the resources-constrained environment is critically impaired. This dependence leads to chronic problems such as unreliable internet connection, power connectivity issues, large data latency making real-time intervention difficulty, excessive bandwidth prices, and, ultimately, piecemeal care of the multimorbid patients. Methods: The study employed the use of a combination of various approaches as it started with an extensive analysis of the current state of telemedicine and its limitation in managing multimorbidity both globally and locally. Then, an architectural framework of a conceptual edge-based framework was designed that defined the primary elements of local data processing, offline functionality, and real-time clinical decision support. Results: This study developed a new, edge-computing telemedical architecture that moves vital data processing and storage operations out of the cloud and on to local edge nodes (edge devices) at the point of care. The main aim was to develop a more robust, effective and responsive telehealth system that will be able to work efficiently even in low-connectivity settings. The possible effect of this framework was compared to the key performance indicators showing that there was a substantial theoretical reduction in the latency of data transmission and the bandwidth used. Moreover, the telemedical model is projected to improve continuity and coordination of care through the processing and acting of critical patient data about IoT devices such as blood pressure, glucose monitoring locally even when the internet is unavailable. Conclusion: Integration of edge computing is a feasible and strategic solution to the basic infrastructural constraints of cloud-based telemedicine in Kenya. The suggested model does not only overcome technical obstacles of connectivity and cost, but also presents a foundational framework of scalable, patient-centered and integrated care to the increasing population of multimorbid patients.},
year = {2025}
}
TY - JOUR T1 - Edge-Based Telemedical Architecture Integrating Edge Devices and Lightweight AI for Healthcare in Kenya AU - Askher Kipkoech Kapkiyai AU - Samson Kabangu Njuki AU - Njeri Ngaruiya Ng’ang’a AU - Isaac Okeyo Y1 - 2025/12/31 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251004.26 DO - 10.11648/j.wjph.20251004.26 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 586 EP - 600 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251004.26 AB - Background: The growing burden of multimorbidity, which is the occurrence of two or more chronic conditions simultaneously in an individual is a great burden on the healthcare system of Kenya that is already defined by unequal distribution of resources and access to specialists. The solution to this gap may be found in telemedicine, but due to the dependency on centralized cloud computing, the effectiveness in the context of the resources-constrained environment is critically impaired. This dependence leads to chronic problems such as unreliable internet connection, power connectivity issues, large data latency making real-time intervention difficulty, excessive bandwidth prices, and, ultimately, piecemeal care of the multimorbid patients. Methods: The study employed the use of a combination of various approaches as it started with an extensive analysis of the current state of telemedicine and its limitation in managing multimorbidity both globally and locally. Then, an architectural framework of a conceptual edge-based framework was designed that defined the primary elements of local data processing, offline functionality, and real-time clinical decision support. Results: This study developed a new, edge-computing telemedical architecture that moves vital data processing and storage operations out of the cloud and on to local edge nodes (edge devices) at the point of care. The main aim was to develop a more robust, effective and responsive telehealth system that will be able to work efficiently even in low-connectivity settings. The possible effect of this framework was compared to the key performance indicators showing that there was a substantial theoretical reduction in the latency of data transmission and the bandwidth used. Moreover, the telemedical model is projected to improve continuity and coordination of care through the processing and acting of critical patient data about IoT devices such as blood pressure, glucose monitoring locally even when the internet is unavailable. Conclusion: Integration of edge computing is a feasible and strategic solution to the basic infrastructural constraints of cloud-based telemedicine in Kenya. The suggested model does not only overcome technical obstacles of connectivity and cost, but also presents a foundational framework of scalable, patient-centered and integrated care to the increasing population of multimorbid patients. VL - 10 IS - 4 ER -
Department of Computing and Information Technology, The Technical University of Kenya, Nairobi, Kenya
Department of Computing and Information Technology, The Technical University of Kenya, Nairobi, Kenya
School of Computing and Engineering Sciences, Strathmore University, Nairobi, Kenya
Department of Health and Biomedical Sciences, The Technical University of Kenya, Nairobi, Kenya
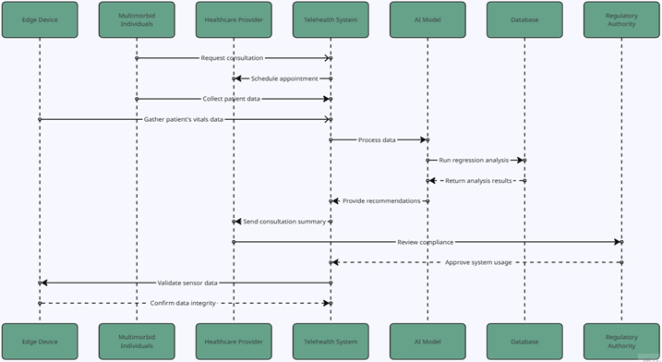
Figure 1. RPM Telehealth System UML Diagram.
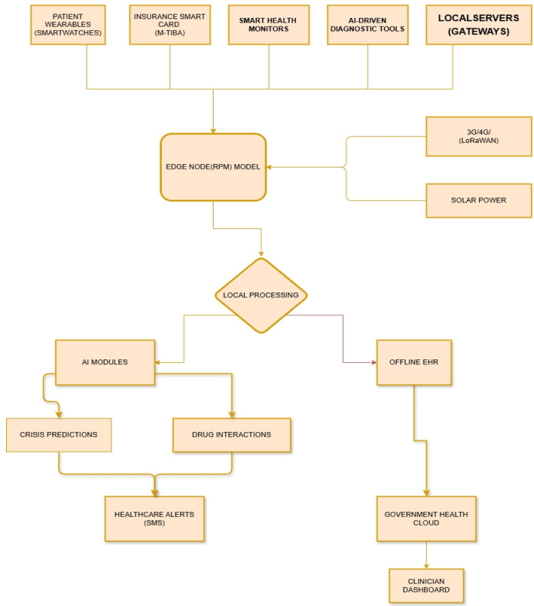
Figure 2. Multi-layered Model Architecture.
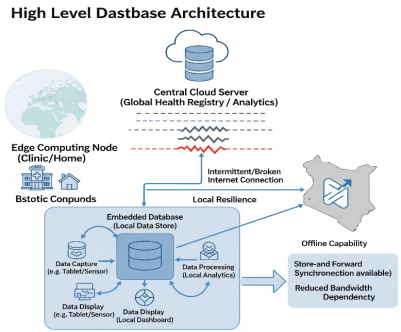
Figure 3. Offline-First EHR Synchronization-Sequence Diagram.
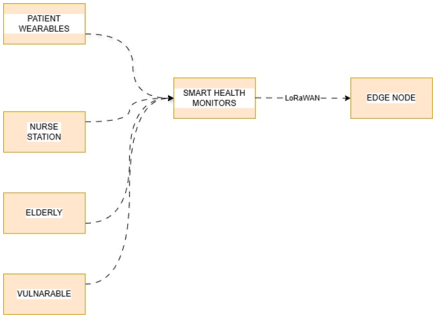
Figure 4. Patient Dataflow Diagram.
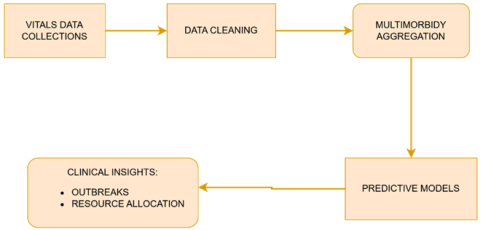
Figure 5. Data Processing and Analysis.
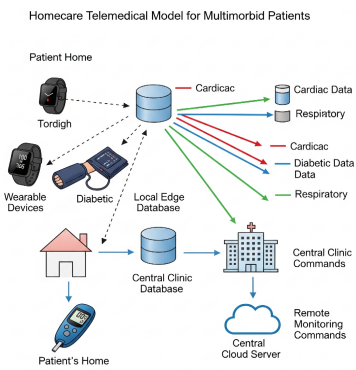
Figure 6. Database Schema Architecture.
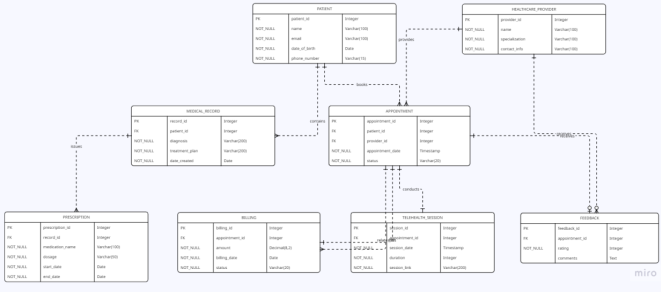
Figure 7. Database Schema.
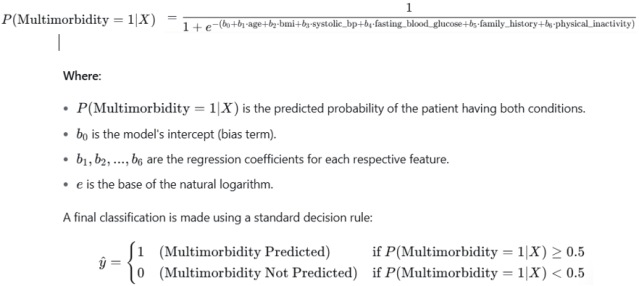
Figure 8. Predictive Model Formula.
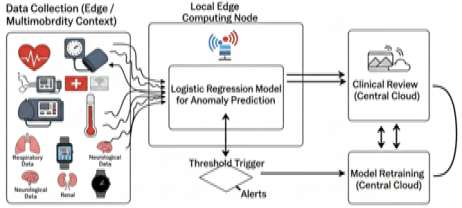
Figure 9. Contextualized Integrated RPM Framework.
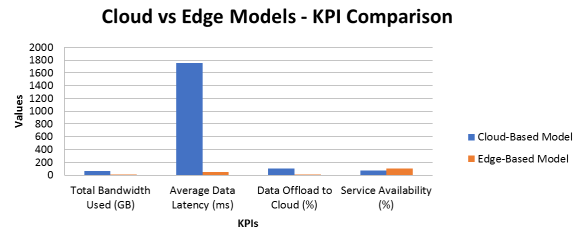
Figure 10. Cloud vs Edge Models - KPI Comparative Performance.
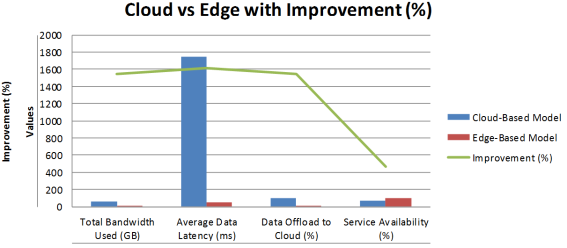
Figure 11. Figure Cloud vs Edge with Improvement (%).

